
The argument for/against legallising euthanasia, medical assistance in dying (MAiD), assisted suicide (or however the legislature wish to brand it) is not something most people are excited to have. For myself it was something I briefly analysed in my youth and, with an arrogant flourish that is known so well to people in their 20’s, decided the conclusion was so obvious as to not warrant further thought or time.
At that time I assumed the only position against assisted dying would be from ignorance steeped in religion; a dark-ages mentality that we, the enlightened and God-free masses would transcend before arriving at a bright, new future where end-of-life suffering was something our children would learn about in history textbooks.
As it is, I grew up and realised that two fundamental truths can be relied upon:
- almost everything was far more complicated than first appeared
- there is nothing in the world that cannot be made orders of magnitude worse by the involvement of government
It is not exactly hard to imagine a healthcare system that could be set poorly devised insentives by a mid-wit management class, resulting in vulnerable people being shuffled towards euthanasia by a monolithic bureaucracy (such as the NHS), is it?
Even in my limited personal experience I have witnessed the NHS kill a patient because of protocol and a concern for meeting targets. And that was without a mechanism to actually do the killing directly. So the idea that it could do so given an actual protocol of euthanasia doesn’t seem like much of a reach to me.
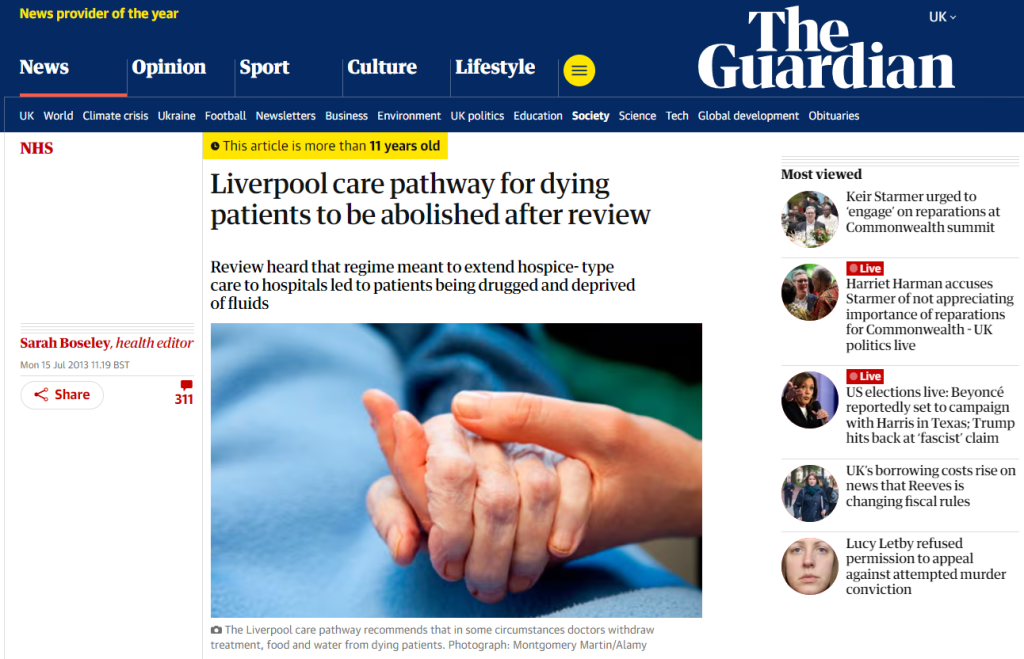
But beyond the annecdotal, a perfect demonstration of a well intentioned end-of-life protocol going rogue was the Liverpool Care Pathway. Much like the proposed MAiD systems, this was a palliative care protocol intended to be used once a patient was assessed as being at the very end stage of life so as to reduce their suffering as much as possible. What it ended up being was a conveyor belt to death which people who weren’t actually dying were shoved on to. Indeed, the care minister at the time of the LCP removal stated:
“I have personally heard families describe staff slavishly following a process without care or compassion and leaving people suffering at the end of their lives. This is something we cannot allow to go on.
In terms of the LCP, the issue wasn’t some group of evil doctors and nurses cackling as they killed the elderly and infirm. The truth is somewhat more worrying. It was just an apparently ubiquitous raft of incompentent medical professionals who slosh around the NHS arbitrarily assigning people as “end of life” and ticking paperwork that meant they were starved/dehydrated to death. These people were murdered by an indifferent bureaucracy in full view of the administration.
But let us move from the annecdotal, beyond the historical parallels and into real world examples. Much like the analysis of the interventions post-Covid, our considerations don’t have to remain entirely hypothetical. We now have Canada to look at in terms of how MAiD systems can be perverted from their original “good” intentions. It’s not looking great and that’s before they expant it to include mental health issues (coming soon).




After a new wheelchair? Maybe you should consider dying. Sorry your care home place isn’t available yet, would you prefer it if we just killed you?
It appears that the biggest safeguarding concern for a MAiD system is not from a disgruntled spouse or pushy children, eager to get their inheretance. It’s your healthcare system who will turn up with a smile (and probably a nice suit) and will kill you on the most vague of assessments.
After COVID it is clear how the establishment wishes arrange the public’s relationship to the national healthcare system; the public serves the NHS and must not burden it and every consdieration of the NHS must be made with those two principles in mind. When we combine this government attidue with the knowledge that the NHS is well staffed with people happy to follow the most abhorrent of orders I have grave concerns for a UK version of MAiD.
